



Experience superior scanning technology with the new Medit i900.


I was a splint blank

The understanding and knowledge of zirconium oxide with regard to the material behaviour and its processing and machining has undergone an evolution in recent years - an evolution towards an aesthetically highly sophisticated dental prosthesis material that is absolutely stable and safe for the end customer.
Dental Direkt GmbH already entered the discussion in 2008 and has published the first compendium with information about the production of the high-performance ceramic zirconium oxide under the above title (Fig.1).
1Titelbild: Zirkonoxid Kompendium von Dental Direkt GmbH, 2008
In the last four years many new and innovative blank types have been introduced to the market in addition to the proven and well documented 3Y TZP types (high-strength, stabilized with 3 mol% yttrium oxide). It is becoming increasingly difficult to maintain an overview of the composition and suitability for the indication. A clear typification and differentiation of the different qualities and material concepts is therefore currently difficult to achieve.
Especially the zirconium oxide ingots, which have been optimized for veneer-free monolithic restorations and whose translucency has been increased, have recently enjoyed growing popularity. In this context, the relationship between increasing translucency on the one hand and decreasing strength on the other hand has been repeatedly discussed in technical articles and at congresses. Super high translucent 5Y TZP (with 5 mol% yttrium oxide approx. 50% tetragonal and 50% cubic crystals are stabilized) have been on the market since about 2014 and the indication is limited to 3-units molar bridges in most cases due to the reduced strength.
However, zirconium oxide has been developed several times - it is undergoing rapid development.
Not all zirconium is the same!

Materials of varying opacity allow the choice for aesthetic lighting management, as this monolithic work in zirconium dioxide shows. This enables attractive solutions for the patient even under different ambient conditions.
Picture: © Anton Sawizki
1. Bending strength
Based on the data sheets and dental technicians, the focus is on bending strength, expressed in megapascals (MPa), as a quality criterion. The bending strength describes how much force is required to deform and ultimately break a test piece with a defined diameter. High values in this discipline are essential for multi-unit restorations. For bridges larger than four elements, a value of 800 MPa must be achieved in a test according to the essential standard for dental ceramics (DIN EN ISO 6872). There can be no doubt that flexural strength is and should be an important quality criterion.
The standard allows a choice of three different test methods to determine the flexural strength. Depending on the test setup, the measured values vary when using the same material. This unfortunate circumstance does not undermine the relevance of the flexural strength as a quality criterion, but requires a further relevant quality criterion in order to allow better comparability in the selection of materials. In addition to the initial strength, fracture toughness (crack toughness) should also be given more attention as a relevant quality criterion.
One could get the impression that the inorganic dental material zirconium oxide has copied from its "organic neighbours". If we look, for example, at the self-healing of bones, in which an autopoietic ability has developed over the course of evolution to repair fresh, microscopically small cracks in a self-healing manner - it seems to be the perfect imitation of a recipe from nature.
This analogy shows that more attention should be paid to fracture toughness as a relevant quality criterion. The KIc - value provides information on how robust a material is, e.g. during processing in the laboratory or during insertion by the practitioner.

The classic, high-strength 3Y TZP zirconium oxide grades are generally characterized by high fracture toughness (>5 MPa√m) - an essential factor for their clinical success. However, as with the flexural strength tests, there are different test methods for fracture toughness. In DIN EN ISO 6872, the test is only a recommendation and not a specification for the manufacturers - there is no obligation to publish it in data sheets.
The phase transition enhancement property of a material is also relevant for the ageing behaviour of a ceramic. The super high translucent 5Y TZP has a lower initial KIc, which is recommended for 3-unit molar bridges with at least >3 MPa√m. The crystalline structure of the 5Y TZP's thus offers little to no potential for phase transformation and thus for reinforcement.
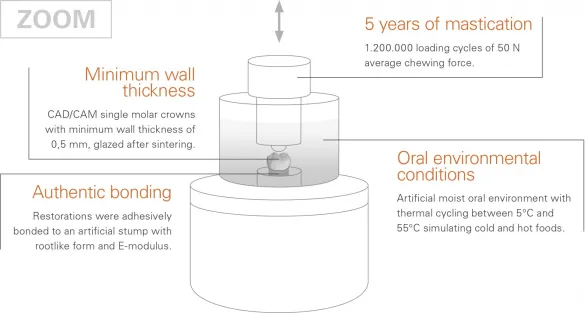
This test set-up simulates the mechanical and thermal loads to which a dental restoration is exposed in the patient's mouth over a period of five years.
The long-term behavior of the material is analyzed in simulated masticatory loading tests (Fig. 4), which show a greater practical relevance compared to standardized material tests. The chewing simulation provides a test procedure that allows reliable conclusions to be drawn about the behaviour of the material in its clinical application. The typical ageing process of a dental restoration in the artificial oral environment is simulated. The crowns are realistically challenged by the influence of moisture and thermal (hydrothermal) alternating stress under mechanical masticatory loading.
In this simulation, eight crowns before and eight crowns of the same type after masticatory loading were destroyed. The force required until failure is measured in N Newton. With a high-strength 3Y TZP (DD Bio ZX²) and a new 4Y TZP (DD cubeONE® ML) with increased translucency, a significant increase in Newton is shown. The mechanical stress of the masticatory load thus leads to a phase transformation that stops the cracks that develop and closes any residual porosity in the ceramic. This increase in stability cannot be observed with the 5Y TZP (DD cubeX²® ML). Although the DD cubeX²® zirconium oxide with a stated flexural strength of 750 - 800 MPa already falls within the range of the required 800 MPa for the ISO 6872 indication "large bridges", it is limited to use for 3-unit bridges due to its lower fracture toughness (KIc >4 MPa√m SEVNB). Within this framework, the high initial values also offer sufficient stability (>1000 N) after the aging process to withstand the maximum force of a bruxist, for example (Fig. 5).
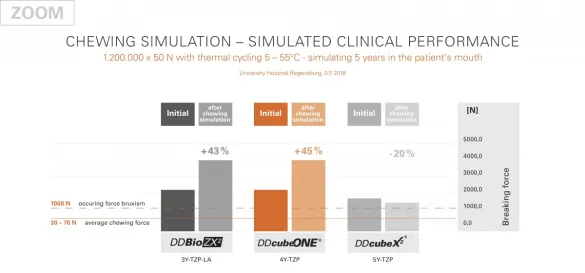
Chewing simulation - simulates a clinical purchase behaviour of 1,200,000 x 50N in thermal cycles of 5-55°C. This corresponds to five years in the patient's mouth. University Hospital Regensburg, 07/2018
DD cube ONE® ML (4Y TZP) has a hybrid crystal structure of about 30% cubic and 70% tetragonal crystals. The KIc is available at ≈10 MPa√m SEVNB. In order to positively influence the aging behavior, aluminum oxide (Al2O3) was added in a balanced concentration. The cubic, large crystals are responsible for the increase in translucency. The KIc value of fracture toughness in the incisal area of the multilayer variant is also as high as in the rest of the body. This is intended to provide the best possible security even in the case of corrections to the occlusal surfaces.
Diversity wins.
Dental Direkt – the complete provider in the dental sector
